|
In the first blog we discussed the health disparities that the Latine community faces, as well as the barriers that go along with these. This includes lack of insurance, language and cultural barriers, and lack of representation in the healthcare field. In the second blog we focused on the latter, emphasizing the lack of Latine healthcare providers and the barriers that our community may face on the healthcare career path. One of these barriers included the lack of representation and knowledge of Latine physicians and researchers. "You can't be something that you don't know about". As our last blog post we wanted to highlight some Latine leaders, healthcare providers, and researchers that have made their mark in the field. We hope that they inspire those into joining the healthcare community and help to continue to reduce health disparities and barriers within the Latine community! Carlos Juan Finlay, MD 1833-1915 Born in 1833 in Cuba, he grew up during the largest outbreaks of yellow fever, a disease that included symptoms like bleeding from the mouth, vomiting, and organ failure. Carlos Finlay saw the fear that surrounded this disease and made it his goal to end it. He graduated in 1855 from Jefferson Medical College in Philadelphia, PA and focused his energy on understanding the cause of yellow fever. After years of ridicule, his finding that mosquitos were the main cause of transmission, the U.S. army eventually followed his recommendation to control the mosquito population. This led to the completion of the Panama Canal. He was praised for his thinking being "the best piece of logical reasoning that can be found in medicine anywhere". José Celso Barbosa, MD (1857-1921) In 1875 Barbosa left Puerto Rico to New York to pursue a career in medicine, which was inspired by a brush with pneumonia. However, officials at Columbia University's College of Physicians and Surgeons rejected his application on the basis that "at a faculty meeting held last night it was decided not to receive students of color". This did not stop Barbosa and he graduated in 1880 from University of Michigan as the first Puerto Rican to receive a medical degree in the United States. His career included caring for soldiers during the Spanish-American War, treating poor patients across Puerto Rico, advocated for a need of employer-based health care insurance, and founded a party that fought for US statehood for PR. He was dubbed the "father of the Puerto Rican statehood movement." Ildaura Murillo-Rohde, PhD, RN (1920-2010) She was known as "The Hispanic whirlwind" for her work as an advocate, nurse, therapist, and educator. She was born in Panama to a family of health professionals. She studied nursing at Medical and Surgical Hospital of Nursing in San Antonio, Texas, graduating in 1948. Murillo-Rohde was shocked to see the limited number of Hispanic nurses serving a large Hispanic population. After graduating, she pursued several other degrees including a PhD from NYU in 1971. Her career ranged from writing about issues from single parenthood to same-sex couples, becoming the first Hispanic dean of nursing at NYU, and creating the National Association of Hispanic Nurses in 1975. Murillo-Rohde's career and advocacy earned her a spot as one of the American Academy of Nursing's living legends. Helen Rodríguez-Trías, MD (1929-2001) Rodríguez-Trías graduated from the University of Puerto Rico School of Medicine in 1970 and soon after began working towards quality care and cultural awareness of minority populations at the Lincoln Hospital in the Bronx as the head of pediatrics. One of the biggest issues that she focused on were the government-led programs that focused on coercing women to undergo sterilization, especially minority women and those with physical disabilities. She co-founded the Campaign to End Sterilization Abuse, which fought for stricter guidelines for consent in 1979. In the 80s she focused her efforts on helping mothers and children who suffered from HIV and/or AIDS, establishing standards of care that became a model for the whole country. She was the first Latina to preside over the American Public Health Association, promoting health equity and women's rights. Before her death she gave her wish "that no one is going to have quality of life unless we support everyone's quality of life." Dr. Jane Delgado, 1953 - present Dr. Jane Delgado was born in 1953, and is a Cuban-American Psychologist, a healthcare advocate, author, and on-profit executive. She was born in Havana, Cuba, and immigrated to the United States with her family to Brooklyn in 1955. Delgado holds an M.A. in Psychology from New York University '75, a Ph.D. in Clinical Psychology from State University of New York at Stony Brook '81, and an M.S. in Urban and Policy Sciences from Stony Brook's W. Averell Harriman School of Management and Policy. She is the author of The Latina Guide to Health, as well as the Buena Salud Guidebook Series. Delgado has worked to promote minority health and the Department of Health and Human Services, making contributions to reduce health disparities and working on the Report of the Secretary's Task Force on Black and Minority Health in 1985. Delgado also led what would later become the National Alliance for Hispanic Health (NAHH), where she served as the first female president, and now serves as the CEO. The NAHH provides service to more than 100 million people in various health related programs. Their most recent campaign being a bilingual one on COVID-19 precautions. Antonia Novello, M.D. 1944 - present Dr. Antonia Novello was born In 1944 in Fajardo, Puerto Rico. The oldest of 3, raised by her mother as her father died when she was 8 years old. As a child Novello was diagnosed with Congenital megacolon, an abnormal dilation of the colon, which should have been fixed early on with surgery. However, Novello would not get this surgery until 18 years later, making multiple trips to the hospital in between. She speaks as this being motivation to study to be a doctor. Dr. Novello has a Bachelor of Science from the University of Puerto Rico in Rio Piedras, and a Doctor of Medicine degree from The University of Puerto Rico School of Medicine in San Juan, and a Public Health degree from Johns Hopkins. Dr. Novello was appointed Surgeon General of the United States by George Bush in 1990, becoming the first woman and Latina to ever have received the honor. In this position she focused on fighting underage drinking and smoking ads that targeted children. She was part of the U.S. Public Health Service Commissioned Corps, worked with the National Institute of Arthritis, Metabolism and Digestive Disorders at the National Institute of Health (NIH). Novello was the Deputy Director of the National Institute of Child Health and Human Development, making contributions in the area of pediatric AIDS. She also helped draft legislation for the Organ Transplantation Procurement Act of 1984. "service is the rent that you pay for living" - Dr. Novello Nora Volkow, M.D. 1956 - Present Nora Volkow was born in Mexico City, Mexico in 1956. She attended the Modern American School and earned her Medical Degree at the National University of Mexico in Mexico City. She is one of the most influential research psychiatrists in the field of substance abuse and addiction, and believes that addiction is a disease. She is the Director of the National Institute on Drug Abuse (NIDA). Her contributions of using brain imaging to drug abuse and addiction has changed this field exponentially, using a PET scan to study people with a cocaine addiction instead of those with schizophrenia and finding changes in blood flow to the prefrontal cortex after 10 days of withdrawal. She was set on this path after going through part of her career watching people suffer from addiction and drug abuse. She saw how the medical field would treat the symptoms, but never attack the root cause to try and solve it. She has changed views on drug abuse being a personal weakness to instead being a brain disease. Serena Auñón-Chancellor, M.D. 1976 - Present Auñón-Chancellor was born in Indianapolis, Indiana in 1976. Her father, a Cuban exile, arrived in the United States in 1960. As a child she always knew she was interested in becoming an astronaut. Auñón-Chancellor holds a B.S. Degree in Electrical Engineering from George Washington University, and an M.D. from the University of Texas Health Science Center at Houston. She first started working at NASA in 2006 as a flight surgeon. She then completed an Aerospace Medicine Residency in 2007 and an M.P.H. at UTMB.
Auñón-Chancellor was the second female Latina NASA Astronaut, and the first Latina female doctor to become a NASA astronaut. She served as Deputy Surgeon for a Space crew in 2009, and was later chosen to be an astronaut, with her first mission in 2012. Since then, Auñón-Chancellor treats patients and trains internal medicine residents at LSU Health Sciences Center in Baton Rouge, Louisiana. She has been treating COVID-19 patients and has stated that the ISS taught her important lessons for handling COVID, self care and teamwork.
0 Comments
Last week, we went over a lot of information on the health disparities that the Latine community faces in the United States. For the second part of MURAL's healthcare series collaboration with UConn Medical School's LMSA, we will address Latine representation, or lack of, in the healthcare field, as well as its importance, barriers to diversity, and ways to improve Latine representation in these fields. Impact of the lack of Diversity Before diving into statistics and numbers, let's discuss the importance of representation and diversity in health care. There are many reasons why diversity should be a priority for health care fields, four of which we believe are vital. These are (1) cultural competence, (2) access for underserved communities, (3) a broadened research agenda, (4) to improve the future management of the healthcare field (Cohen, Gabriel & Terrell, 2002). Diversity in the healthcare field would lead to a culturally competent workforce. By 2050, more than 50% of the United States will be Latine/Hispanic, Black, Asian, or multi-racial. This pushes for a need for a health care force that understands the communities they are serving. By cultural competence, we mean the "knowledge, skills, attitudes, and behavior required of a practitioner to provide optimal health care services to persons from a wide range of cultural and ethnic backgrounds'' (Cohen, Gabriel & Terrell, 2002). Health care providers have to understand what different belief systems our communities have, and how to help them while treating their illnesses. Cultural competency is not something that can be learned from reading books. To achieve it, health care providers must be in environments of whichever diverse community they will serve to interact with individuals from different ethnic and racial backgrounds. This is made more effective by having people from these very same diverse communities within the providers, helping others understand. Access for underserved populations will also be improved with a more diverse health care field. The United State's health professions shortage areas are those that are populated predominantly by Black and Latine/Hispanics. Members of these communities who do gain access to health care often receive lower quality care and face discrimination, whether biased or not, when being treated. Data shows that Black, Latine/Hispanic, and Native American physicians are more likely than white physicians to practice in underserved communities, and to treat more minority patients regardless of their income (Cohen, Gabriel & Terrell, 2002). We also know that when patients and health care providers share racial and/or ethnic backgrounds there is a higher rate of satisfaction for patients. This data suggests that a more diverse health care field would reduce the lack of access for minority communities in the United States. 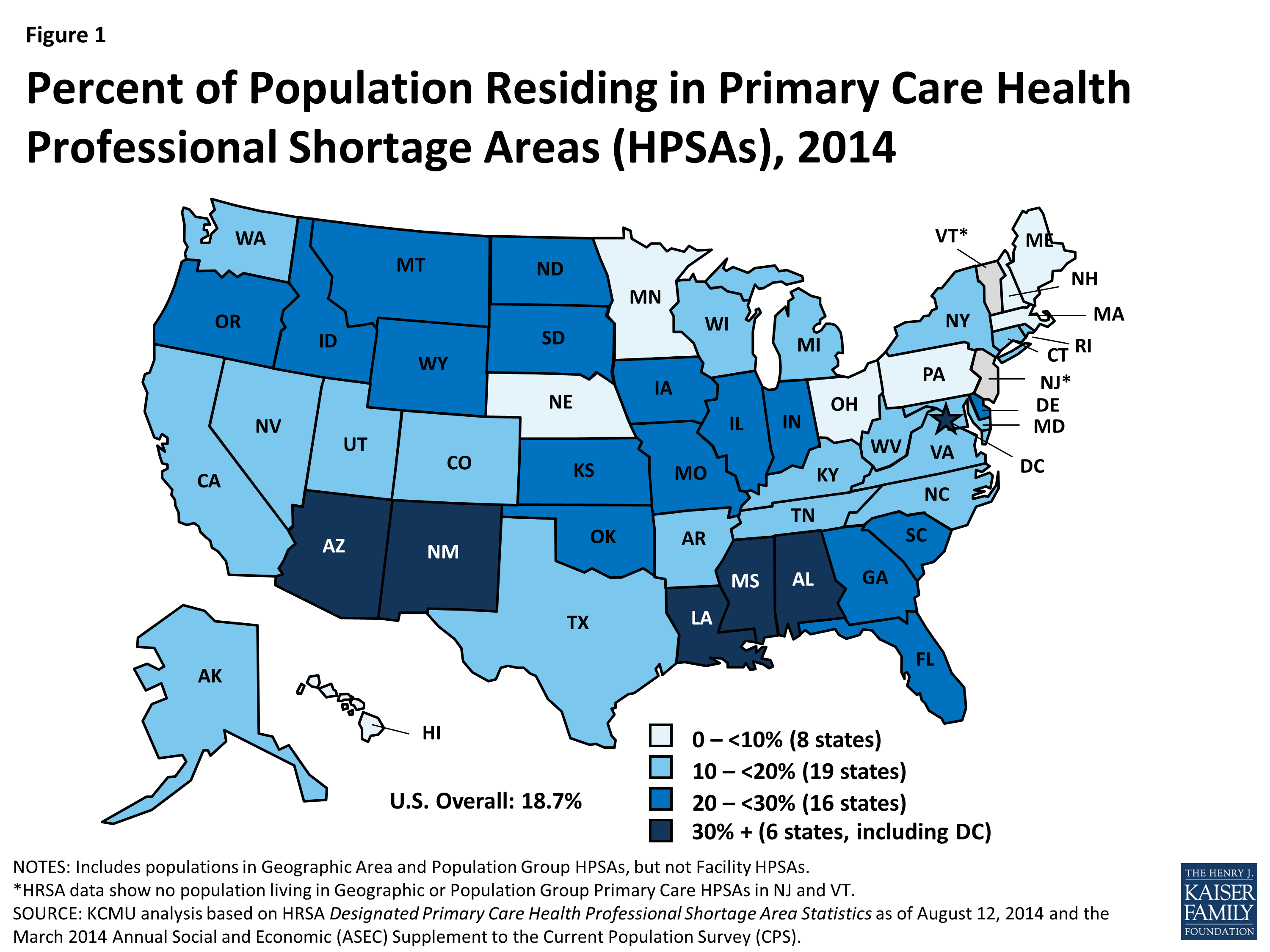 Increased representation would create more advocates for broadening health research. As we learned in the first section of the health care series Latines are disproportionately affected by unsolved health problems. There is a strong need for medical research in these fields, but not enough of a push for them despite the large number of the U.S. population that suffers. This research would also include trials, and to have successful trials there would need to be participation from the Latine general public. Having health care providers that share ethnic and racial backgrounds would encourage more people to trust in this process and partake in studies. Lastly, diversity in health care professions would increase the amount of Latine representation in related health care administration jobs. Policy makers and medically trained executives are crucial to managing the health care system. They hold the power to influence governmental efforts that address health care issues in U.S. populations. Therefore having people who reflect the populations they serve, Latine, Black, Asian, and Native American, would be beneficial in leading future efforts towards the right path that helps those they are meant to serve. Current Number of Latines in Healthcare in the United StatesNow let's dive into some numbers. In the figure below, you can see that the majority of applicants to medical school for the academic year of 2018-2019 were white (49%), compared to 6.2% for Hispanic, Latine or of Spanish origin. This came to a total of 3,297 Latines applying for medical school in that year. 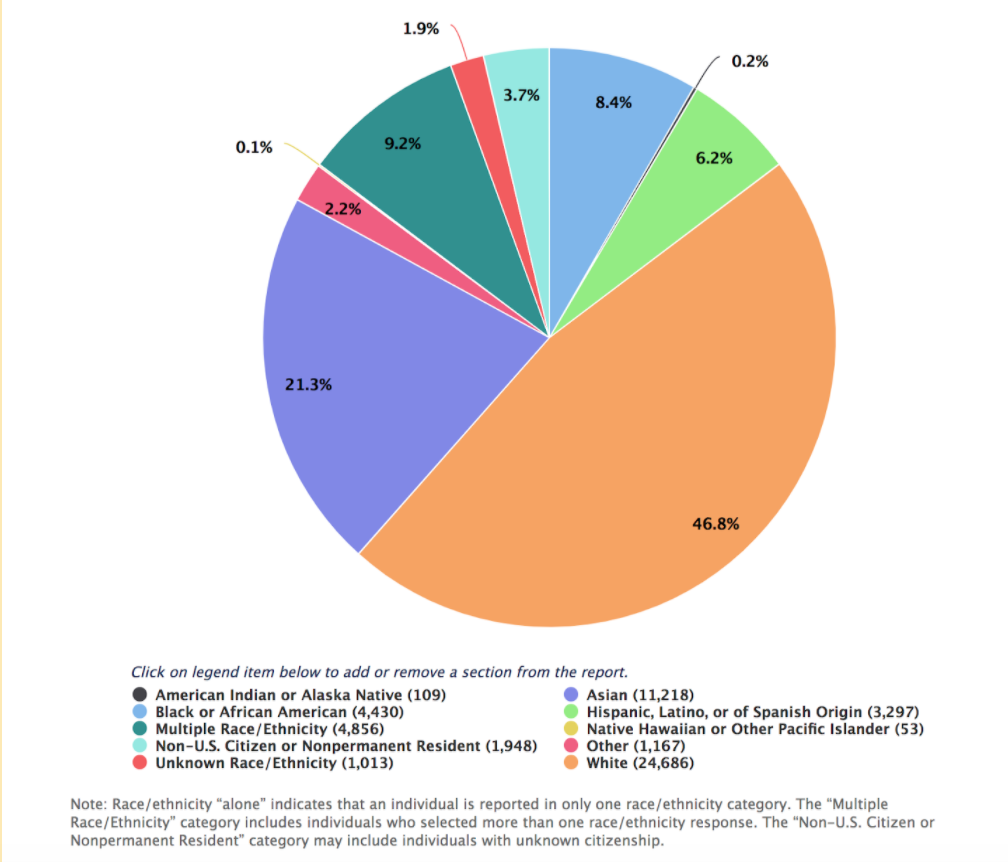 Figure 1: Percentage of applicants to U.S. medical schools by race/ ethnicity (alone) in the academic year of 2018-2019 (AAMC Applicant Matriculant Data File). The figure below breaks down what the backgrounds of the 3,297 applicants look like. 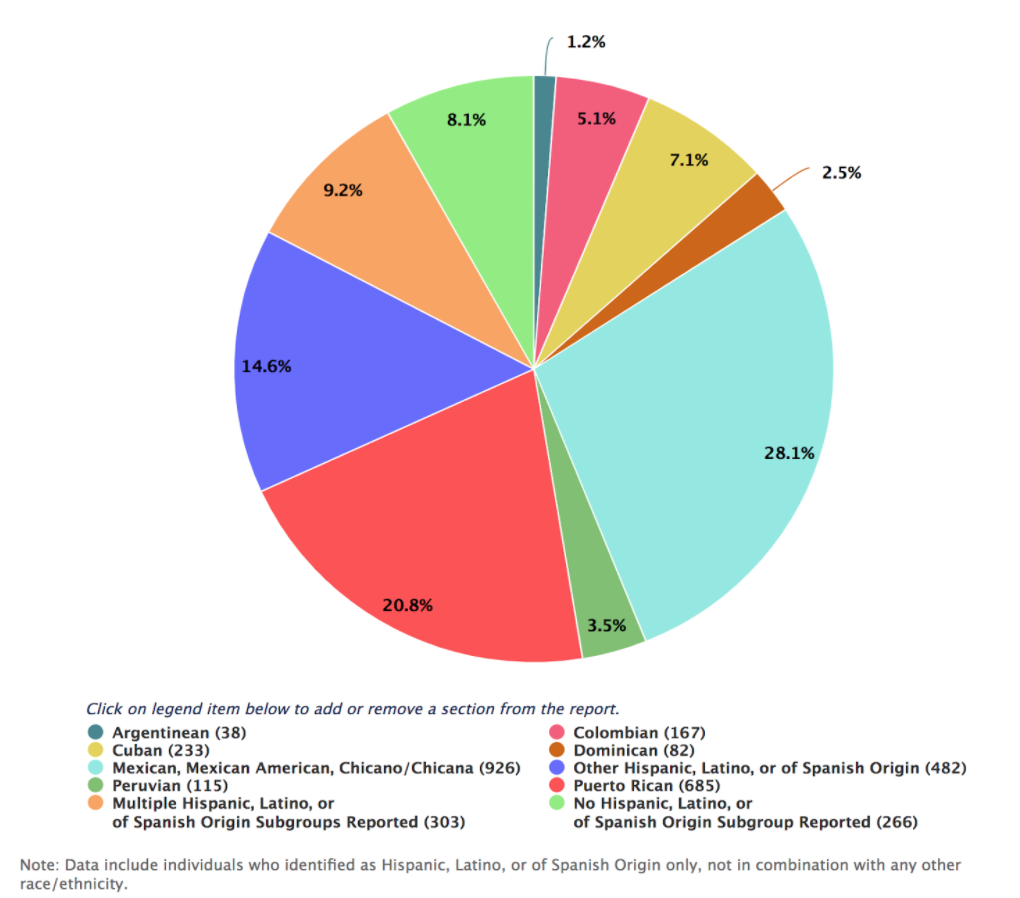 Figure 2: Percentage of Hispanic, Latine, or of Spanish origin (alone) applicants to U.S. medical schools by subgroups for the academic year of 2018-2019 Looking closer at medical schools, we see that 63.9% of full-time faculty were white, with only 3.2% of full time faculty being Latine in the same academic year. Even more distressing, the percentage of active physicians in 2018 for whites was 56.2% compared to the 5.8% of Latines. In numbers, this is a total of 516,304 white doctors compared to 53,526 Latine doctors for the entire United States Population. Clearly, there is a deafening lack of Latine representation in physician positions. Barriers for Underrepresented Minorities in Health ProfessionsThe lack of representation in the healthcare field is due to a wide range of barriers. UCSF did a literature review to identify the key barriers. One of the most prominent barriers was the financial cost of entering the healthcare field. Minorities are more likely to have lower socio-economic status, with the median income for Latine households being $47,675 compared to $64,041 for non-Latine White households. This has a huge impact on student's ability to attend 4-year colleges, with 48% of qualified students not going because of financial barriers. In addition, the length of schooling worsens the financial barrier. To receive a medical degree to be a physician, students must attend school for 8 years, meaning many will accumulate debt for those years and no way to pay it off until graduation from medical school. In addition to financial barriers, underrepresented minority (URM) students are less likely to be prepared for the rigorous class load due to weaker high school classes. As a result, they typically have lower GPAs in undergrad, lowering their chances for medical school admissions which are strongly based on GPA and standardized test scores. Additionally, URM students are less likely to access admission test resources due to how expensive these can be. The underrepresentation in medicine alone is a barrier, as there is a lack of mentors for these students. One individual in the study emphasized this point: “One thing medical school is good at is beating you up…if you have mentors that look like you, it’s a sign of hope and is very powerful.” Having racially diverse mentors helps students balance their academic and social needs. In addition, students may feel like they may have to "prove themselves" because of stereotype threat. Being one of the few minorities in the classroom can make one feel uncomfortable and feel the need to show they "deserve to be there". This can have a huge impact on if a student feels mentally prepared to go to a graduate program, despite having all the criteria to be successful. Most importantly, the lack of exposure to health care careers plays a huge role. You can't become what you don't know. Most families don't have doctors in their social networks and if you only have contact with healthcare professionals when you go to your doctor, then you aren't going to be aware of the opportunities that the career has to offer. In addition, they may have difficulty accessing internships which are a huge part of the admissions process. This is added to by poor advising. Pre-health advisors are often unaware of resources for URMs, and often discourage students with low grades from applying, which as stated previously impacts minority students greatly. Ways to Increase RepresentationAfter knowing these barriers it is important to address them to increase URMs in healthcare fields. The earliest intervention can be in elementary and high schools with large minority populations. There are several programs where students from health professional programs and health professionals volunteer to talk with these students and teach them about the many healthcare career opportunities. This early exposure introduces interest at a younger age and helps students develop goals.
There are also institutional changes that should occur in each institution to increase support for minority students: Academic support: Tutoring, admissions test preparation, summer enrichment programs Emotional support: Access to counseling services, workshops for families Financial support: Scholarships, paid internships, loan repayment, assistance with child-care and transportation Social Support: Peer, faculty, alumni, and community mentorships These also include building bridges between high schools with large URM populations and colleges to help support the transition into rigorous coursework and improve grades. Lastly, as representation increases in the healthcare field and increase in important mentorship will increase as well, helping students on their career path. Organizations like LMSA also help greatly. LMSA is an org founded to represent, support, educate, and unify US Latine medical students. Located all over the country it aims to provide mentoring, a voice, leadership, advocacy, and volunteering within the Latine community. This includes helping high schools students, pre-med undergraduates and medical students. To learn more about the mission and opportunities of LMSA visit http://national.lmsa.net/. MURAL has partnered with UConn Medical School's Latino Medical Student Association (LMSA) to create a 3 part healthcare series for our audiences. In this first part of the series, we will be discussing health disparities faced by the Latine community. Before we get into this, as some of you may know, MURAL has decided to replace "Latinx" with "Latine". For more information on this decision, please check out our official announcement on Instagram here. As many of us are aware, Latines in the United States face healthcare disparities as a community, including higher risks of diabetes and obesity, and faring worse in access to health insurance. While we have a lower death rate overall, we also have a 50% higher death rate from diabetes according to the CDC. Latines have a higher chance of developing type 2 diabetes, more than 50%, and are even more likely to develop it at a younger age. This means the Latine community is also more likely to develop the consequences stemming from diabetes, like kidney failure and vision loss. According to the CDC, Latines living in the United States are 17% more likely to develop type 2 diabetes compared to non-Hispanic White Americans. Puerto Rican's are twice as likely to develop type 2 diabetes compared to those from South American backgrounds. Moreover, Mexicans and Puerto Ricans are almost twice as likely to die from diabetes compared to non-Hispanic White Americans. Just this past year, the CDC declared Diabetes as the 5th leading cause of death for Latines in the United States. 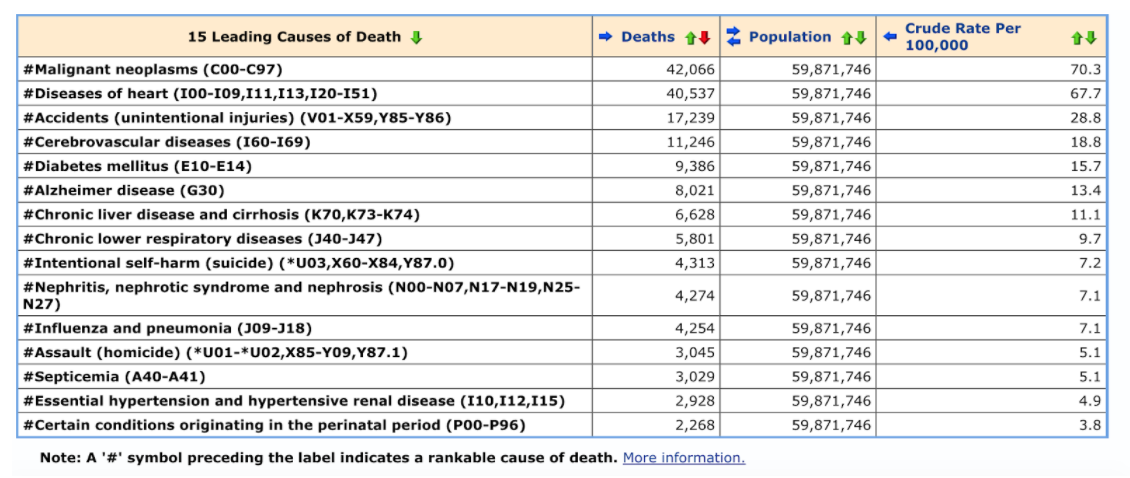 Figure 1. 15 Leading Causes of Death for Latines in the United States, as per the CDC. Click the picture to access the CDC source. There are different categories for obesity, Grade 1 being overweight, Grade 2 being obesity, and Grade 3 being severe or morbid obesity. These categories however use BMI to differentiate who fits where, which is based off of white Caucasians, and varies by race, therefore being an inaccurate measure for communities of color. Regardless, this is what we have to work with at the moment. Knowing this, data from the CDC shows that 11.3% of Latines in the U.S. are Categorized as Grade 2 Obese compared to 9.4% non-Hispanic white Americans. 25.7% of Latines in the U.S. are categorized as Grade 1 Obese, compared to 20.5% non-Hispanic white Americans, and 44.8% Latines are categorized obese compared to 27.4% non-Hispanic white. We also want to talk about the large disparity in health insurance that the Latine community faces. In 2017, 49% of Latines had private coverage compared to the 75.4% for whites. Keep in mind that if you have no coverage, you are less likely to go to a doctor. According to the CDC, 20.9% of Latines under the age of 65 were uninsured in 2018, compared to 10.9% whites under the age of 65, and 12.2% for Black Americans. In this same year, 3.7% of Latines over the age of 65 were uninsured compared to 0.6% Whites over the age of 65, and 1.3% for Black Americans. Moreover, Latines at or under the poverty line were more likely to be uninsured, at 33.6%, compared to Whites at or under the poverty line at 15.1%, and Black at 18.2%. This is more than double the chance to be uninsured for those at or under the poverty line compared to whites. "If you have no health insurance coverage, you are less likely to go to a doctor" Circumstances That Lead to These DisparitiesThese health risks are higher in Latines for a variety of reasons. This includes diet! The wide variety of cultures in the Latine community have many different diets that impact health. Beef, pork, rice and beans, fried foods, high amounts of starches and oils, and large portions all influence a person's risk of developing heart disease or diabetes. Our diet is important to us, we love to have family dinners and clean our plates. However, making healthier choices will help prevent the onset and progression of health problems. Swapping out fried foods for healthier baked options, making smaller portions, and swapping out double serving of rice for vegetables could all be healthy swaps. We don't have to get rid of our favorites! Just be more aware of how we are eating them. According to the CDC, these diets additionally impact children greatly. Latine children and teens are at a higher risk for type 2 diabetes. Having unhealthy eating habits as a child increases your risk of developing diabetes, heart disease, and weight problems, more than as an adult. In addition, it makes it a lot harder for them to change diets as an adult when they do start having health problems. Starting these healthier changes at a younger age is essential in preventing these diseases from developing. Language has always been and remains to be a barrier that contributes to these health disparities in Latine community have when interacting with providers. 6 in 10 Hispanic adults have reported having a hard time communicating with a health care provider, because of language or cultural barrier (Swanson & Contreras, 2018). If a patient can't communicate with their physician, how are they expected to personally address their health problems? Having interpreters is essential in providing care, but many providers try to avoid interpreters to save time and money. By law, every patient has the right to request an interpreter, and it is important that more patients are aware of this. Culture Plays a Part in the Latine Health Care ExperienceOur culture also plays a big part in our health. Although Latines themselves have varying cultural practices, we do share similarities between each other. Carteret mentions fatalismo, referring to how some Latines believe we as individuals have little say in altering our fate. This impacts our health, as Latine patients are more likely than white patients to believe having a chronic disease, such as cancer, is incurable, or a punishment from God. Many would prefer not to know if they even have such an illness, and are less likely to seek preventive screenings, or delay visiting a doctor when symptoms are severe (Carteret, 2011). Our cultures also affect our diets, which in turn affects our health. Dietary behaviors are of the first things to be influenced by acculturation when an immigrant starts adopting the norms of the new country they are in. This is suspected to be correlated with diabetes and obesity rates in Latines (Cuy Castellanos, 2015). Environmental factors also affect dietary changes as the U.S. offers more processed and canned foods compared to traditional fresh ingredients Latines use for traditional dishes. Geographical location also influences access they have to these ingredients, along with prices and freshness. Cuy Castellanos is quick to point out that while this may be a trend, it is not applicable to all Latines as we are diverse in our cultures.  In the U.S. there is a focus on biomedical and curative approaches to medical treatment, with not a lot of holistic body and mind approaches. Because of this, Latine services like santería are seen as less qualified, which leads to a condemnation of alternative or complementary services. The Latine community would benefit from education on U.S. medical approaches, as well as how to pair it with their own accepted medical approaches, which the U.S. has unfortunately deemed "traditional or folklore" (Holliday, 2008). In the states, public health officials see culture and tradition as barriers that block Latines from accessing proper health services. Their teams are set up to shut down "illegal folklore" practices, which sends a message to the Latine community that what they have done in their home countries in terms of health care is wrong (Holliday, 2008). Moreover, there is a belief in the U.S. that Latine immigrants are taking American jobs, creating anti-immigrant sentiment. Because of this, some uninsured Latine immigrants seeking health services face strained relationships with medical providers, fearing deportation (Ransford et. Al, 2010). In terms of health care seeking, data shows that Latines use a mix of biomedical health care services from the U.S. when affordable, as well as alternative medicine like botánicas. Latines interview by Ransford and his team stated they turned to herbal medicines when they didn't have access to the biomedical ones. How Can Providers Help?Cultural competency is essential for providers to have. Cultural competence is the ability to understand, communicate with, and effectively interact with people across cultures.
How can we be culturally competent health providers? 1. Provide interpreter services 2. Recruit and retain minority staff 3. Provide training to increase cultural awareness, knowledge, and skills 4. Coordinate with traditional healers 5. Use community health workers 6. Incorporate culture-specific attitudes and values into health promotion tools 7. Include family and community members in health care decision making 8. Locate clinics in geographic areas that are easily accessible for certain populations 9. Expand hours of operation 10. Provide linguistic competency that extends beyond the clinical encounter to the appointment desk, advice lines, medical billing, and other written materials Most importantly, as health providers, we have to ask questions! It is never okay to assume someone's health and needs based on their cultural background. Knowing the cultural differences is important, but we never know how an individual identifies or interprets their culture so asking questions will be the best way to help patients. SOURCES Carteret, M. (2011, March). Cultural Values of Latino Patients and Families . Dimensions of Culture Cross-Cultural Communications for Healthcare Professionals. Retrieved March 18, 2012, from http://www.dimensionsofculture.com/2011/03/cultural-values-of-latino-patients-andfamilies/ Cuy Castellanos, Diana 2015. Dietary Acculturation in Latinos/Hispanics in the United States Heymsfield, S. B., Peterson, C. M., Thomas, D. M., Heo, M., & Schuna, J. M., Jr (2016). Why are there race/ethnic differences in adult body mass index-adiposity relationships? A quantitative critical review. Obesity reviews : an official journal of the International Association for the Study of Obesity, 17(3), 262–275. https://doi.org/10.1111/obr.12358 Holliday, Karen V. 2008. “Folk” or “Traditional” versus “Complementary” and “Alternative” Medicine” Constructing Latino/a Health and Illness through Biomedical Labeling. Ransford, H. Edward, Frank R. Carrillo, Yessenia Rivera. 2010. Health Care-Seeking among Latino Immigrants: Blocked Access, Use of Traditional Medicine, and the Role of Religion. Obesity Classifications: https://www.medscape.com/answers/123702-11460/what-is-the-who-obesity-classification-system#:~:text=Grade%201%20overweight%20(commonly%20and,equal%20to%2040%20kg%2Fm https://www.cdc.gov/nchs/data/hus/2018/026.pdf https://ftp.cdc.gov/pub/Health_Statistics/NCHS/NHIS/SHS/2018_SHS_Table_P-11.pdf https://www.cdc.gov/vitalsigns/hispanic-health/index.html https://www.cdc.gov/diabetes/library/features/hispanic-diabetes.html https://hpi.georgetown.edu/cultural/ https://www.aarp.org/health/conditions-treatments/info-2018/latinos-hispanics-doctors-nursing-homes.html#:~:text=Nearly%206%20in%2010%20Hispanic,Center%20for%20Public%20Affairs%20Research https://www.cdc.gov/diabetes/library/features/hispanic-diabetes.html |
AuthorsPaula Norato - MPA Student at The University of Connecticut, with a Bachelor of Science in Molecular and Cell Biology, minor in Latino Studies. ArchivesCategories |
 RSS Feed
RSS Feed
